

He is sitting in his car outside the pharmacy, the engagement email from some clinic still open on his phone. Free consult. No labs required. Ship next day. It sounds like exactly what he wanted six months ago, when the fatigue and the flat mood first made him start Googling at 1 a.m. It also sounds like a shortcut around the one thing that actually protects him.
That tension, between wanting relief now and needing someone to check the work, sits at the center of every testosterone decision a man makes. This piece is not here to talk anyone into or out of TRT. It is here for the moment after that decision starts to feel real, when the question stops being “should I” and becomes “who do I trust with this.” Good hormone care leaves a paper trail: labs, doses, follow-up, written down somewhere a person can point to. If a provider cannot produce that trail, that is the whole answer, right there.
One thing worth separating out before anything else. Choosing a provider is not the same job as deciding whether testosterone belongs in your body. That second question only your bloodwork, read by a clinician, can settle. This is about the first job, and doing it right gives the second job an actual chance to be answered honestly.
The question nobody wants to ask first
Before comparing prices or reading a single testimonial, there is one question worth sitting with: is this a confirmed low-testosterone reading, or is it a feeling of being run-down that testosterone has become shorthand for?
It matters more than it sounds like it should, because the entire safety case for treatment is built on that answer. The Endocrine Society’s guideline is specific about it: hypogonadism should be diagnosed only in men who have both symptoms and an unequivocally low testosterone reading, confirmed by repeating a fasting morning measurement rather than acting on a single number [1]. The FDA draws the same line, approving testosterone products for hypogonadism tied to a medical condition, and stating plainly that benefit and safety have not been established for low testosterone that comes simply from aging [5]. A clinic willing to prescribe off a symptom quiz, no real bloodwork involved, has already skipped the first move of the standard of care. That is not efficiency. That is the tell.
And if the labs come back normal, the more honest answer might be that testosterone was never the fix. A provider worth keeping will say so. One that sells anyway has told you everything you need to know.
What oversight is supposed to look like, in practice
Every clinic says “medical oversight.” Almost none define it, so here is the version worth checking for.
A licensed clinician reads the history and the labs before anything gets prescribed, and that same person, not an algorithm, sets the starting dose and adjusts it later. There is a human to reach when something changes. The medication itself comes from a licensed pharmacy, not a shipment from a chemical supplier. And the relationship does not end at the first order, because the guideline calls for structured monitoring through the first year, rechecking testosterone, hematocrit, and prostate risk [1]. A provider that takes payment, ships a vial, and never asks for a second blood draw has failed the most basic definition of oversight, no matter how good the app looks.
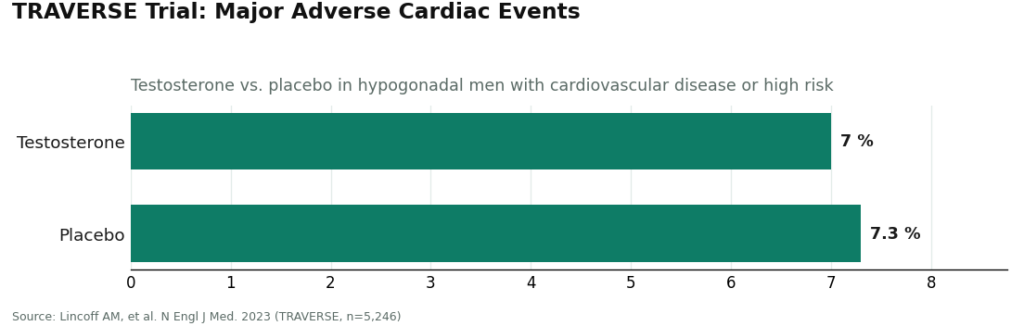
That is not a hypothetical concern. TRAVERSE, the large cardiovascular trial built to answer this exact question, was reassuring on the headline number: testosterone was noninferior to placebo for major adverse cardiac events, 7.0 percent versus 7.3 percent [3]. But the same trial recorded higher rates of atrial fibrillation, acute kidney injury, and pulmonary embolism in the men on testosterone [3]. Those are precisely the things a clinician doing real follow-up is supposed to be watching for. Oversight is not a formality bolted onto the process. It is the mechanism built to catch what the data says to expect.
What responsible dosing actually looks like
There is no single “right” dose to hand someone, and any provider offering one universal number is telling on itself. What responsible dosing looks like is a pattern, not a figure.
It starts low and moves according to labs and symptoms, not a fixed protocol. It tracks hematocrit, since testosterone can thicken the blood by raising red-cell count, which is exactly why a complete blood count sits inside the guideline’s monitoring plan [1]. It watches estrogen too, since some testosterone converts to estradiol, and swings in either direction cause their own problems. And it is honest about what the treatment can and cannot deliver. In the Testosterone Trials, men with genuinely low levels saw real improvement in sexual activity, desire, and erectile function, with a modest lift in mood, but no significant benefit for vitality on a standard fatigue scale [2]. A provider dosing someone toward an energy promise the data never supported is selling a feeling, not treating a diagnosis.
One habit protects a patient through all of this, and it costs nothing: keep your own record. Log the injections, the dates, how the week actually felt, so every follow-up conversation starts with something concrete instead of a vague impression. Some supervised programs build a version of this in. The FormBlends tracker app, for example, is a dose and symptom logging tool that lets a patient hold onto exactly that kind of history over time. It is not a prescription and there is no checkout attached to it, just a way to walk into a clinician’s office with real data instead of guesswork. Notebook or app, the principle does not change: the paper trail belongs to the patient too, and it is what makes the oversight actually function.
The conversation almost nobody starts on their own
This is the part most men do not think to raise, which is exactly why it needs to be said plainly. Standard testosterone therapy suppresses the body’s own production, and that can lower sperm count and fertility. Anyone who might want children later is not dealing with a footnote here. It is a decision point, and a provider who does not bring it up on their own has skipped a real part of the job.
The encouraging news is that the field actually has answers for this, which is itself a reason to favor a provider carrying more than one option. Enclomiphene can raise a man’s own testosterone by stimulating the pituitary. In a randomized trial against a topical gel, it matched the gel’s effect on testosterone while raising LH and FSH and conserving sperm counts [4]. HCG, used alongside testosterone or during recovery afterward, keeps the testicles functioning. A 2025 real-world analysis found it lifted the share of androgen-suppressed men reaching a normal total motile sperm count from 5 percent to 58 percent, though not every man in the study got there [6]. A provider that only sells straight testosterone has no way to route a patient toward either option. Raise fertility plans at the very first visit, and judge the provider partly on whether they had already thought to ask.
One honesty note worth carrying into that conversation: enclomiphene is not FDA-approved. It is prescribed and prepared through compounding pharmacies under a valid prescription, and a provider worth trusting will say that outright rather than letting it sound like an approved drug [5].
A short list worth checking before paying anyone
Stripped down to what can actually be verified before money changes hands, a provider worth trusting does all of the following. It requires real bloodwork and confirms low testosterone before prescribing anything, rather than working from a questionnaire [1]. It keeps a licensed clinician in charge of choosing and adjusting the dose, with medication filled at a licensed pharmacy. It commits to follow-up labs over time, not a single shipment and silence [1]. It asks about fertility goals and can offer enclomiphene or an HCG protocol, not testosterone alone [4][6]. It is honest about the benefits, sexual function and mood, not a vitality cure [2]. And it says plainly when something is compounded and not FDA-approved [5]. Miss two or more of those and the answer is already clear.
The route worth actively avoiding is the research-chemical one, and it is worth being blunt about why. A vendor shipping testosterone or HCG labeled “research use only” screens nothing, sets no dose, monitors nothing, and answers for nothing about what is actually in the vial. That label is not a technicality. It is the seller telling you, in writing, that none of the safety steps above apply to what you are about to inject. The molecule inside might be identical to a prescribed version. Everything that makes it safe to use is missing.
Where a supervised model actually fits
For anyone who would rather have this checklist already assembled than build it piece by piece, FormBlends is one provider that sits inside that category. A clinician reviews the patient profile first, a prescription only follows that review, and anything prescribed comes out of a licensed 503A compounding pharmacy rather than an unregulated warehouse. This gets mentioned once here, as an example of what the supervised-access model looks like in practice, not as a ranking and not as a claim about cost or outcome.
What compounding alone does not hand anyone is the thing this whole guide keeps circling back to. The paper trail. A history someone actually read, lab numbers that steered the decision, a pharmacy that can be held to a standard, and follow-up testing that changes the plan when the plan needs changing.
Where this leaves the guy in the car
The protection is not complicated, even if it takes some patience to apply. Pick a provider that confirms a real diagnosis, keeps a clinician attached to the dose, follows up with labs, raises fertility before you have to ask, and tells the truth about what testosterone does and doesn’t do. Keep your own log of doses and symptoms so the follow-up conversation has something real to work from. And refuse, outright, the channel that skips all of it.
Good hormone care leaves a paper trail. If none is visible, that is not the provider to use. The next move is straightforward: find a licensed clinician, get the bloodwork done, and build that trail together, one appointment at a time.
Testosterone, enclomiphene, and HCG are all prescription treatments, and enclomiphene along with any compounded preparation are not FDA-approved finished drug products. That is a fact worth carrying into the room, not a reason to avoid it.
The questions that keep coming up
What is the single biggest red flag in a TRT provider?
The clearest warning sign is a provider willing to prescribe from a symptom questionnaire with no blood test behind it. The standard of care diagnoses low testosterone only when symptoms line up with an unequivocally low reading, confirmed by a repeated fasting morning draw, so skipping that step means skipping the first safety gate, not saving anyone time [1]. Without real bloodwork before the prescription, nothing else about the offer matters much.
Can a legitimate TRT prescription actually come through telehealth?
Yes, and telehealth TRT can be entirely legitimate as long as the oversight stays intact underneath the convenience. The real test is whether a licensed clinician reviews labs and history, whether an actual pharmacy dispenses the medication, and whether the program brings the patient back for follow-up testing instead of shipping a vial and disappearing. A slick app is not the problem. An app with no clinician and no repeat labs behind it is.
How often should a good provider recheck bloodwork on testosterone?
A responsible provider rechecks through a structured first year, looking at testosterone level, hematocrit, and prostate risk, then keeps monitoring on an ongoing basis after that [1]. The hematocrit check matters because testosterone raises red-cell count and can thicken the blood, and trial data also flagged higher rates of atrial fibrillation and clotting events worth watching for [3]. A one-time shipment with no second blood draw fails this test completely.
What should someone ask about fertility before starting testosterone?
Ask whether the provider can offer a fertility-sparing route before committing to anything, since standard testosterone suppresses the body’s own production and can lower sperm count. Enclomiphene raised testosterone comparably to a topical gel in a randomized trial while preserving sperm parameters, and HCG can help maintain or restore production, so a provider stocking only straight testosterone cannot route a patient to either [4]. Raise family plans at the first visit and judge the provider partly on whether they had already asked.
Why avoid “research use only” testosterone or HCG from a vendor?
Because the “not for human use” label is a legal disclaimer signaling that every safety step has been skipped. A research-chemical vendor screens nothing, sets no dose, monitors nothing, and stands behind nothing about what is actually in the vial. The molecule may match a prescribed version exactly, but the screening, dosing, and follow-up that make it safe to inject are precisely what is missing.
Is it a problem that enclomiphene is compounded and not FDA-approved?
Not on its own, as long as the provider says so plainly. Enclomiphene is prescribed and prepared through compounding pharmacies under a valid prescription, and even FDA-approved testosterone products are indicated for hypogonadism tied to a medical condition rather than ordinary aging [5]. What is worth watching for is a provider implying a compounded preparation is an approved drug; clear disclosure is the signal to trust.
References
- Bhasin S, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2018. Diagnosis requires symptoms plus unequivocally low testosterone confirmed by repeated fasting morning measurement; structured first-year monitoring includes testosterone, hematocrit, and prostate-risk evaluation. https://pubmed.ncbi.nlm.nih.gov/29562364/
- Snyder PJ, et al. Effects of Testosterone Treatment in Older Men (The Testosterone Trials). N Engl J Med. 2016. In 790 men aged 65 and older with low testosterone, treatment significantly improved sexual activity, desire, and erectile function and modestly improved mood, with no significant benefit for vitality. https://pubmed.ncbi.nlm.nih.gov/26886521/
- Lincoff AM, et al. Cardiovascular Safety of Testosterone-Replacement Therapy (TRAVERSE). N Engl J Med. 2023. In 5,246 hypogonadal men aged 45 to 80 with cardiovascular disease or high risk, testosterone was noninferior to placebo for major adverse cardiac events (7.0 percent vs 7.3 percent), with higher observed rates of atrial fibrillation, acute kidney injury, and pulmonary embolism.
- Wiehle RD, et al. Enclomiphene citrate stimulates testosterone production while preventing oligospermia: a randomized phase II clinical trial comparing topical testosterone. Fertil Steril. 2014. Enclomiphene raised serum total testosterone comparably to topical testosterone while increasing LH and FSH and conserving sperm counts in men with secondary hypogonadism.
- FDA Issues Class-Wide Labeling Changes for Testosterone Products. U.S. Food and Drug Administration. Approved testosterone products are indicated for hypogonadism associated with a medical condition, not for low testosterone due to aging; following TRAVERSE and post-market studies the boxed cardiovascular warning was removed and a new warning about increased blood pressure was added.
- Smit DL, et al. Efficacy of human chorionic gonadotropin hormone in restoring spermatogenesis in men using non-prescribed androgens: a retrospective analysis of real-world data. F&S Reports. 2025. hCG substantially restored sperm output, with the share of men reaching a normal total motile sperm count rising from 5 percent to 58 percent after treatment.
How much does a legitimate TRT clinic actually cost, and what should that price include?
Expect somewhere around $100 to $200 a month at a reputable clinic once the consultation, medication, and basic monitoring are all factored in. Be wary of rock-bottom pricing that leaves out follow-up labs, since a cheap upfront fee often just means paying separately for every blood draw and check-in call later. A fair price bundles at least quarterly labs, access to the provider for questions, and dose adjustments without surprise invoices showing up afterward.
How can someone tell a TRT clinic is legitimate before handing over a credit card?
A legitimate clinic requires either a physical exam or a genuinely thorough intake history, orders baseline bloodwork before prescribing anything, and can name the licensed pharmacy filling the prescription. It is worth checking that the prescribing physician holds an active, unrestricted state medical license, which is free to verify through a state medical board website. If a clinic skips labs, pushes for a same-day decision, or cannot say where the testosterone is compounded, those are serious warning signs worth taking seriously.
What is the real difference between a men’s health TRT clinic and just asking a primary care doctor?
A primary care doctor can absolutely prescribe and manage TRT, and for straightforward cases that is often the most coordinated option, since they already know the patient’s full health history. Specialty men’s health clinics tend to move faster, offer more flexible dosing schedules, and sometimes carry a wider formulary, including options like enclomiphene or HCG alongside testosterone. The trade-off is that a siloed clinic may not communicate well with a cardiologist or endocrinologist already in the picture, so bridging that gap may fall on the patient.
Is a compounding pharmacy a reliable source for testosterone, or is brand-name the only safe option?
Compounding pharmacies that are licensed and PCAB-accredited can be a reliable, sometimes more affordable, source, particularly for formulations that are not commercially available, like certain cream strengths or subcutaneous pellet alternatives. The key is accountability: the prescription should flow from a licensed physician through a verifiable pharmacy, not through a website selling vials with minimal paperwork attached. Some physician-supervised programs, FormBlends among them, use this compounding route in a structured, trackable way that mirrors the oversight standards built around brand-name prescribing.
Written by Quinn Ellison, freelance health reporter. Last reviewed June 2026.
For readers’ general information. Medical decisions belong with you and a licensed professional.



